A 45-year-old recreational golfer visited the Sports Medicine Department at Ortho One with a frustrating complaint. For several months he had been experiencing sudden tremors and jerky wrist movements while putting during competitions. What was once simple and easy became unpredictable. He complained of stiffness in his hands and momentarily freezing before striking the ball. Interestingly, he could practise normally on the driving range but in a competition setting he lost control entirely. The condition had begun affecting both his performance and his confidence adding several extra strokes to his game.
After an evaluation, the symptoms were identified as the yips, which involves involuntary muscle activity during precise movements. He gradually returned to competitive sport after a rehabilitation program that focussed on relaxation and motor retraining.
This guide is written for both athletes and clinicians. It covers the full picture from what the yips are, why they happen, how they are diagnosed and how sports medicine treats them effectively.

The yips are involuntary disturbances of fine motor control that occurs during well-learned movements. Athletes involved in golf, archery and shooting may experience tremors, jerks and spasms that interfere with smooth and coordinated action. The yips often occur in high pressure, competitive settings but the movement feels entirely normal in lower-pressure contexts.
The yips can be seen in athletes competing in golf, shooting, cricket, baseball, darts, and archery. It can affect both professional and recreational athletes who have highly trained fine motor skills and experience performance pressures.
The yips occur during competition due to psychological pressure and an underlying vulnerability. The most clinically significant feature of the condition is its pressure-specific nature.
The yips is diagnosed by careful evaluation by excluding other movement disorders and identifying sport-specific triggers. The diagnosis is structured and objective and done in a way to understand the athlete's full history.

A detailed clinical history helps determine when the problem started and whether symptoms differ between practice and competition. The clinician finds out the onset of the yips, when it occurs, previous injuries, psychological stressors and current symptoms. This history is sufficient to make a strong diagnosis and indicate which classification of yips the athlete has.
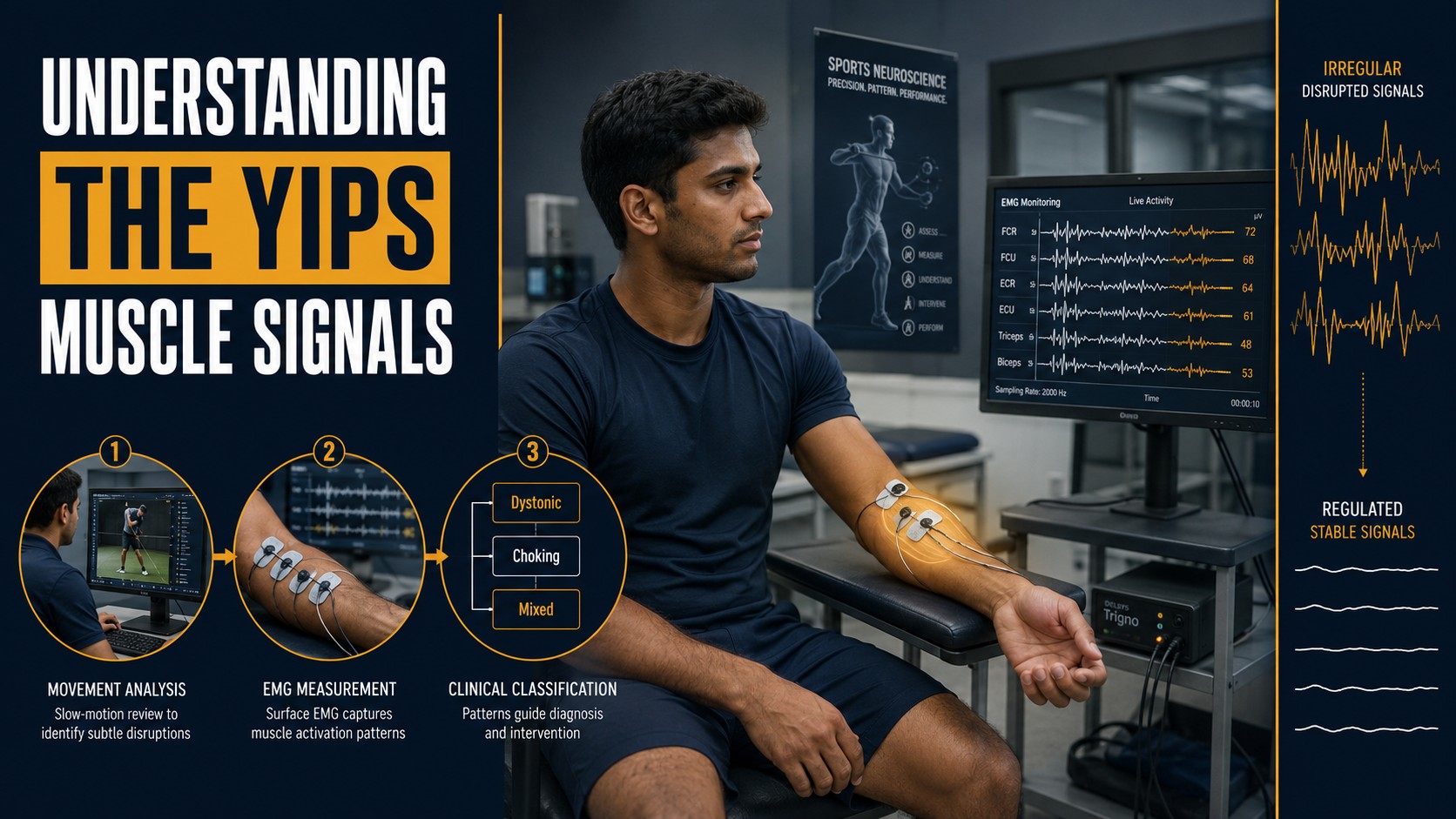
Video analysis allows clinicians to view subtle jerks or freezing movements that are not visible during a routine examination. Slow-motion footage of the athlete can reveal the precise moment and nature of the motor disruption. Electromyography provides objective evidence revealing abnormal muscle co-contraction patterns. Psychological assessment helps identify stress, attention and anxiety that triggers the condition.
The yips are classified into dystonic, choking and mixed type. The dystonic type is predominantly neurological. The choking type is predominantly psychological and the mixed type is caused due to neurological and psychological factors. This classification allows clinicians to guide treatment decisions, by determining whether the focus should be primarily on motor retraining, psychological intervention, or a combination of both.
Athletes affected by the dystonic-type benefit from sensorimotor and neuromuscular retraining. They may require medical interventions such as botulinum toxin in severe cases. Athletes affected by the choking-type respond well to anxiety management techniques, attention retraining and gradual competitive re-exposure. Athletes with the mixed-type benefit from a fully integrated programme. Accurate classification at the outset prevents mismatched treatment and shortens the road to recovery.
Managing the yips focuses on restoring smooth and automatic movement in high-pressure situations. The treatment aims at retraining the coordination between the brain and muscles while reducing excessive muscle tension.

Sensorimotor retraining helps athletes regain accurate body awareness and make precise movements. Slow-motion practice helps to reduce the speed at which errors occur allowing the nervous system time to re-learn correct sequencing. Sensory cueing uses tactile, auditory, or visual stimuli to guide movement by avoiding faulty automatic patterns. Graded motor imagery involves mentally rehearsing the movement in realistic scenarios without physical execution, recalibrating the brain's motor map before the body attempts the action again. Together, these sensorimotor retraining techniques normalise movement patterns and reduce involuntary contractions that define the yips.
Neuromuscular retraining focuses on improving muscle coordination, helping athletes reduce abnormal co-contraction and develop more efficient motor strategies.
Biofeedback tools allow athletes to observe their own muscle activity in real time, identifying when and where excessive tension occurs. Athletes learn to consciously reduce that tension and with sufficient practice it becomes integrated into their automatic movement patterns.
Athletes are encouraged to try varying grips and postures to encourage flexibility in movement patterns. This action prevents the rigid motor habits that are closely associated with the development of focal dystonia. This approach may feel counterintuitive to athletes accustomed to seeking consistency, but it is an important part of the neuromuscular recovery process.
Motor control is rebuilt gradually, beginning with low-pressure drills and progressing to full sport simulation. This staged approach prevents the anxiety and pressure of competition from undermining the gains made in rehabilitation before the athlete is ready.
Rhythmic cues such as metronome pacing can significantly improve movement timing and reduce sudden freezing episodes. Athletes can bypass the over-conscious deliberation that causes freezing by anchoring the movement to an external rhythm. This rhythm is internalised over time and the movement regains its fluency and automaticity.
Manual techniques may be used to reduce muscle tension and improve joint mobility, enhancing proprioceptive input and motor control. Physiological relaxation techniques such as diaphragmatic breathing and progressive muscle relaxation help reduce background muscle tension and improve steadiness during performance. Attention is also given to proximal stability such as poor trunk or shoulder control. Correcting these foundations often produces meaningful improvements in fine motor control.
When symptoms are severe or persistent and do not adequately respond to rehabilitation alone additional medical treatments may be considered. These decisions are made on an inpidual basis by the sports medicine physician who takes into account the classification, severity, and overall clinical picture.
In focal dystonic cases where specific muscles are over-contracting, involuntarily carefully targeted botulinum toxin injections may reduce the abnormal contractions and improve movement control. This allows the athlete to gain a window in which correct movement patterns can be re-established and consolidated through rehabilitation.

Recovery from the yips rarely occurs through a single intervention. Improvement usually comes from a combination of technical adjustments, motor retraining, and regulation of physiological stress. Many athletes experience meaningful improvement with inpidualised care, although recovery timelines vary. Some athletes see significant progress within a few weeks while others require several months of sustained effort.
Early recognition and appropriate management improve the chances of a successful return to performance. The longer the condition goes unaddressed, the more entrenched the abnormal motor patterns and the psychological associations become. Psychological stigma and under-recognition remain significant barriers as many athletes hesitate to report performance difficulties, and many clinicians are unfamiliar with the condition.
Many athletes achieve full or near-full recovery with appropriate treatment. Whether this constitutes a permanent cure depends on the inpidual, the underlying cause, and how comprehensively rehabilitation addresses both the neurological and psychological components.
No! Choking under pressure is a psychological phenomenon that can affect any athlete in any skill. The yips is a psycho-neuromuscular condition that involves measurable changes in muscle activity, is task-specific, and can have a significant neurological component. Choking may contribute to or overlap with the yips but the two are not the same.
Yes! With structured sports medicine rehabilitation, the majority of athletes with the yips can return to their sport and to meaningful performance. The golfer in our opening case study returned to playing comfortably and regained confidence in his game. Early diagnosis, appropriate management, and a commitment to the rehabilitation process are key factors.
An athlete should seek help as soon as the pattern becomes noticeable and is affecting performance or confidence. The earlier a sports medicine specialist evaluates the condition, classifies its type, and begins a structured rehabilitation programme, the faster and more complete the recovery.
Consult our sports medicine physician today.
Address
Operational Hours:
10:00 AM – 7:00 PM | Monday to Saturday
Facilities
Treatments
Quick Links

 Book an appointment
Book an appointment Athletes Empowerment
Athletes Empowerment Orthopaedic Education
Orthopaedic Education